This is one of those articles that may (hopefully) help define a new era of medical education!
Charles Prober (senior associate dean at Stanford SOM and author of the article “Lecture Halls Without Lectures”) and Salman Khan (creator of the Khan Academy) have co-authored an editorial calling for “a collaborative, multi-institutional effort to reimagine medical education.” This “reimagining” recognizes that the current medical system is generally inflexible to individual learners and embraces the flipped classroom model at it’s core.
They argue that the convergence of 3 key factors compels a need for change:
- The modern “digital native” learner
- Exponentially growing biomedical knowledge
- A dated medical education delivery system
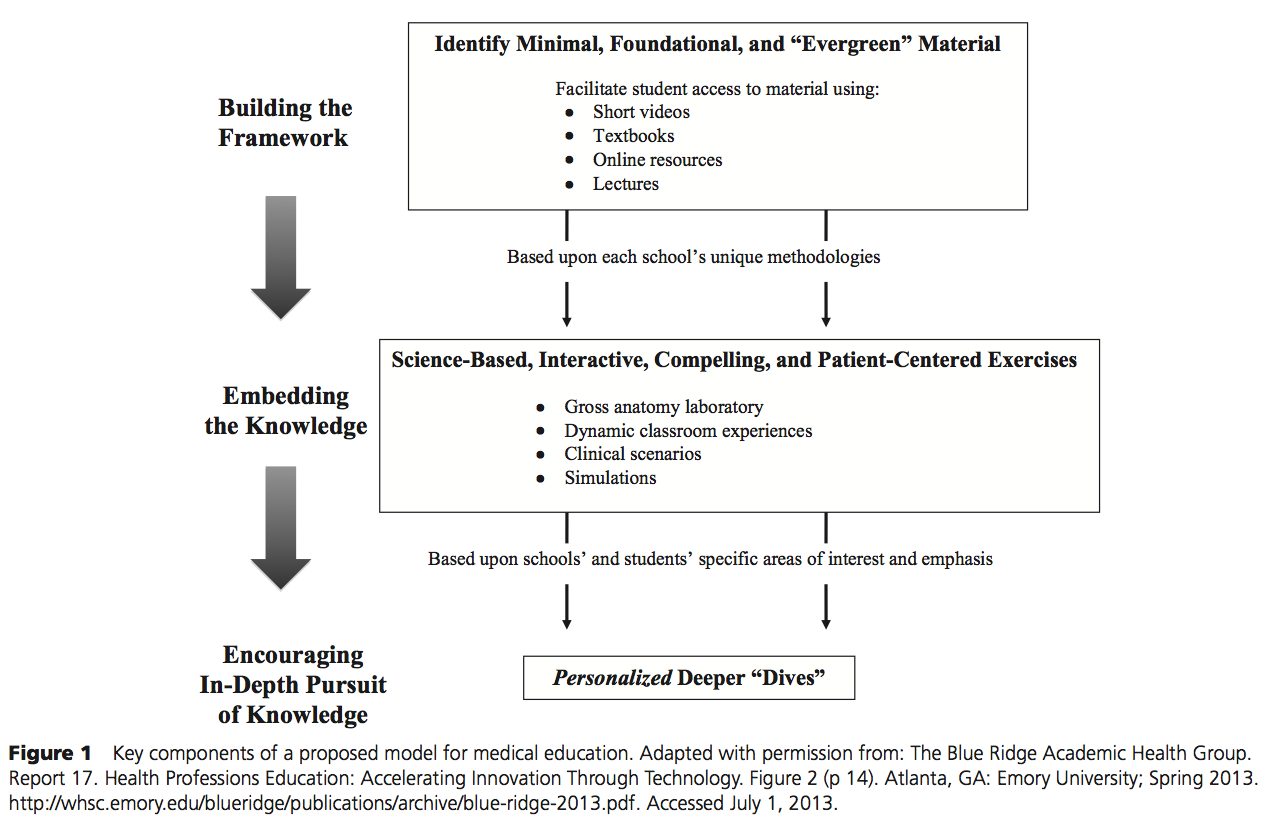
To do this, they propose the following:
 (Click to enlarge)
(Click to enlarge)
Building a framework of core knowledge
This is the central element of the proposal and calls for a curricular change to focus on medical knowledge that is “evergreen,” or foundational and known to be true. They then call for the creation of a medical school collaborative to identify the core content, and based on this, to create short (~10 minute) videos of this core content.
Embedding the knowledge in richly interactive, compelling, and engaging formats
Interactive, engaging sessions add meaning to the knowledge and solidify the learners understanding of the material. Based on the experiences at Stanford, they also note that the sessions with video-based didactic instruction must be time neutral compared to the current model.
Encouraging in-depth pursuit of knowledge in some, but not all, domains
Here, the key is “to tap into and support the individual learner’s aptitude and passion.” Deeper “dives” into the curriculum and driven by learners and areas of expertise in each school. It also respects that some students may not feel the need to do so.
This commentary is rich with ideas to embrace technology and the flipped classroom model for our learners. It is a model that was developed for K-12 education, but as the authors note, equally relevant to medical education. There are also several keys to this model which I think are worth mentioning more in depth:
- Collaboration – it calls for medical schools to work together to define a core content across all schools
- Embracing technology – using technology not only for the core content, but also the interactive sessions to reinforce key ideas and material
- Encouraging multiple formats – recognizing that there will need to be several videos formats to fit various learning styles.
- Individualism – while collaboration is key to this endeavor, medical schools maintain individualism in the style and delivery of the interactive sessions and the areas of expertise for the “deep dives” offered to students
- Tailored education – students may (or may not) choose to go beyond the curriculum in “deep dives” in certain areas
I am energized by this article and excited to be an educator right now!
References
Prober C, Khan S. “Medical Education Reimagined: A Call to Action.” Academic Medicine. 2013;88(10):1-4