(Click image to go to site)
(Click image to go to site)
I get asked very often about Prezi as a presentation tool. Thought it would be worthwhile to write about it.
Prezi is a cloud-based presentation design tool that uses zooming and “paths” to move through the presentation instead of the standard slides. It is a great way to create digital stories and change the pace from the normal slide-based presentation software. One of the most impressive features of Prezis is the ability to go off the path and explore any part of the presentation at any time. This feature lends itself extremely well to medical education, as we are sometimes locked into a set path because of inability to deviate from the set order of our slides (although there are a few way to address this).
I’ve used Prezi for a few presentations now. Below is an example of one of my VERY early Prezis as well as a few other great ones.
(Click on images to view Prezis and make sure to explore the features while viewing)
Innovations in Educational Technologies
(this one is mine, as you will quickly be able to tell. Did I mention this was an early attempt?)

.
Social Media in Medical Education

.
Honoring Dr. Martin Luther King

.
Prezi Pros vs Cons
Pros:
- Completely different from standard, slide-based software
- Ability to deviate from the “path” and create or explore anywhere in the presentation as needed
- Extremely powerful for persuasion type presentations
Cons
- Very, very steep learning curve (you have to really invest the time to make them great)
- Very time intensive (this improves with time just like any other software)
- Potentially nausea inducing (sometimes, people get a little overzealous with the spinning functions)
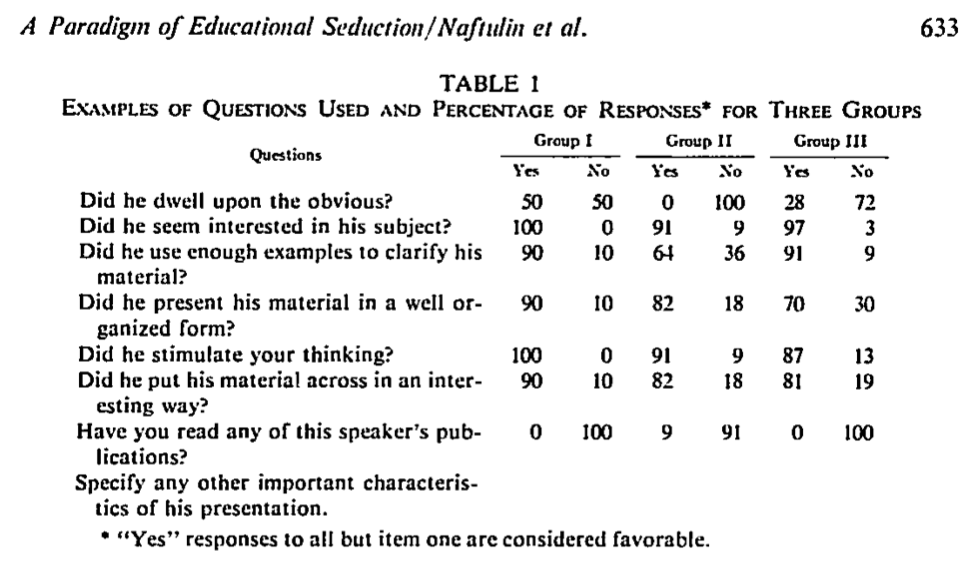
The bottom line: Prezi is a great presentation software platform, but has a huge learning curve, and still doesn’t make up for the good ol’ design principles you have come to know and love. Without understanding and incorporating educational design principles, it will be a great visual feat with no content (similar to the “Dr. Fox effect”).
I’m interested in your opinions on Prezi as educators, specifically in medical education. How have you used it in your teaching? What other opinions do you have about it? If you are willing to share, please reply to the post or send a message to @designformeded using the Twitter box on the right.